Photograph by Iris Johnson
By Palmer R. Cook, OD
Benjamin Franklin did not wear wrap (or face form) frames even though the wind flowing across a kite flier’s eyes can promote dryness. He had quite an eye for the ladies, but he never had the stylish look that wrap frames can provide. Poor Ben—he didn’t know what he was missing.
Actually wrap or face form frames have both practical as well as cosmetic advantages. They can block UV by decreasing back-surface reflections of ultraviolet light. They can be very effective in blocking light that enters the pupil at an oblique angle, which is thought to be one reason that many patients form early coronal cataracts in the nasal periphery of the crystalline lens. Certainly they reduce air currents that evaporate the water layer of the corneal tear film, particularly when the oil layer of tear film is compromised. Wrap frames can be effective in eliminating foreign bodies from the peripheral environment. Most of all, at least from patients’ viewpoints, a wrap frame can look very “cool,” and they are often patient-preferred for cosmetic reasons.

Wrap frames can be cosmetically pleasing, but they must also function well. The lenses mounted in a wrap frame are rotated around a vertical axis (Fig. 1). When viewing a wrap frame from above, it is apparent that the right lens is rotated in a clockwise direction, and the left lens is rotated in a counterclockwise direction. For a frame with a total 20-degree wrap, each lens is rotated 10 degrees. This means that the lines-of-sight, when the patient is looking straight ahead at a distant object, are passing through each lens at an 80-degree angle instead of a 90-degree angle. This obliquity has certain optical consequences. For low power prescriptions and for frames with only a little wrap, these consequences can usually be ignored.
 Ophthalmic laboratories since Ben Franklin’s day have traditionally ignored the issue of frame wrap for frames with small amounts of wrap, and they “lay out” lenses as though the lines-of-sight pass through them at a right (i.e., 90 degrees) angle (Fig. 2). This works pretty well when the lens power is low, and when the frame wrap is 5 to 6 degrees or less, which is about average for the frames generally considered to be non-wrapped. Our lensmeters are equipped with holders that place the lens’ surfaces at a right angle to the operator’s line-of-sight or the sensors in the case of auto-lensmeters. Objective and subjective refractions are customarily done with the patient’s lines-of-sight at right angles to the lens’ surfaces.
Ophthalmic laboratories since Ben Franklin’s day have traditionally ignored the issue of frame wrap for frames with small amounts of wrap, and they “lay out” lenses as though the lines-of-sight pass through them at a right (i.e., 90 degrees) angle (Fig. 2). This works pretty well when the lens power is low, and when the frame wrap is 5 to 6 degrees or less, which is about average for the frames generally considered to be non-wrapped. Our lensmeters are equipped with holders that place the lens’ surfaces at a right angle to the operator’s line-of-sight or the sensors in the case of auto-lensmeters. Objective and subjective refractions are customarily done with the patient’s lines-of-sight at right angles to the lens’ surfaces.
What worked well for over a century was a system of examining with test lenses at right angles to the lines-of-sight, fabricating eyewear as though the lenses were to be worn so the lines-of-sight passed through the lenses at right angles and analyzing lens powers with light paths at right angles to the lens surfaces. Today there are countless wrap frames that hold the lenses rotated around a vertical axis. In spite of all of the advantages of wrap frames, prescription and even plano lenses do not perform well if they are fabricated and analyzed in the “traditional” manner.
 WRAP INDUCED PRISM
WRAP INDUCED PRISM
When a light enters lenses that have been rotated around a horizontal axis (i.e., pantoscopic tilt), a prism effect is generated (Fig. 3). Because both lenses are rotated in the same direction (bottom-inward, top-outward), a “yoked prism” effect is generated that produces base down prism. This prism is of little importance since the bases are in the same direction, and the amount of prism is usually about the same in both eyes. However, this pantoscopic rotation is very important for other reasons, as every dispenser knows. With a wrapped frame, the lenses are rotated in opposing directions, one clockwise and the other counterclockwise. This creates a prism effect that is base out in either eye. It is dependent on the power of the front curve of the lens so lenses with steep front curves generate more prism, and those with flatter front curves generate less prism. For lenses with plano front curves, no prism is generated.
Odd as it may seem, this prism effect is independent of the lens power although the index of the lens material and the thickness both have an effect. For a +8.50 front curve, an index of 1.49 and a thickness of 2.5 mm and a 9-degree rotation (wrap) for each lens, the lens would have a prism effect of about 0.29rBO (Fig. 3). Grinding in an opposing prism can compensate for this, but you may have to remind your lab to do the calculations and compensations (i.e., in this case adding 0.29r of BI prism to each lens). If the wrap were increased to 13 degrees, the induced prism would increase to about 0.33rBO in each lens. Manufacturers of high-end, plano, wrap sunglasses make this prism accommodation because they have found that their customers notice and appreciate the improved optics.
 WRAP INDUCED DECENTRATION CHANGES
WRAP INDUCED DECENTRATION CHANGES
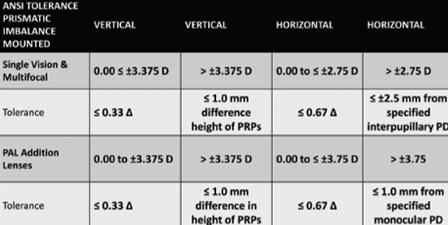
As mentioned above, labs typically lay out lenses as though both lenses are in the same plane. In fact, most frames have some wrap, and this causes the MRPs or Distance Reference points to move closer together (Fig. 4). This effect can be demonstrated by creasing a sheet of paper down the middle. When the paper is folded along the crease, the outer edges move closer together. The angle of wrap displaces the MRPs or optical centers of the lenses in the same way. In order for your patient’s lines-of-sight to line up with the MRPs or the Distance Reference points correctly, they must be decentered outward by an amount that is dependent on the degree of wrap and the PD. For narrower PDs, smaller degrees of wrap and lower power prescriptions, the Rx PD variance from the anatomical PD may not be problematic, but when the PD and degree of wrap are greater, the variance may cause unacceptable prismatic effects depending on the power of the lenses (Table 1).
 MEASURING WRAP
MEASURING WRAP
As with all pre-ordering measurements, the frame must be fitted before the measurements are taken. It’s a good idea to note the wrap measurement and be sure it is unchanged when the finished job is returned to you. It’s usually easy to return a frame to its original wrap by modifying the bend in the bridge. Because the lab will use your wrap measurements in calculations, a failure to dispense the frame with the same wrap will result in less than optimal lens performance. Wrap can be measured in various ways including a wrap template chart (Fig. 5), as well as with more sophisticated electronic tools.
 MEASURING THE FINISHED EYEWEAR’S PD
MEASURING THE FINISHED EYEWEAR’S PD
Of course, wearing a wrap frame does not change anyone’s anatomical PD. It’s just that your lab may need to center your patient’s lenses differently to give the maximum benefit of the lens technology that was prescribed and ordered for them. Using an inexpensive plastic Boley gauge with a millimeter scale is an easy and practical way to check the MRP or Fitting Cross separations on finished eyewear (Fig. 6). Another way of measuring is to lay a PD rule on the eyewear so that it is parallel to a straight line joining the two points you are measuring; however, since you are measuring a wrap frame, there will be a gap from the PD rule to the points you are measuring, and it will be difficult to get an accurate measurement because of parallax. The quick and easy way is to use a Boley gauge as shown in Fig. 6.
It is also possible to estimate the half PDs using the Boley gauge, but a truly accurate half-PD measurement is difficult. This is because the location of the center of the bridge must be estimated, and if the gauge is held correctly with the bar between the jaws of the gauge parallel to a line connecting the points being measured, the tips of neither jaw will be in contact with the lens or any part of the frame. Fortunately, as long as the full PD is correct, small errors in the half PDs should not be problematic. If your patient has one half PD that is more than 2 mm greater than the other, consult your lab about the advisability of fitting a strongly wrapped frame.

DIGITAL TECHNOLOGY
Digital lens technology has made the performance of prescription lenses in wrap frames better than ever. In part, this is due to the ability of digital lathes to tailor the unique curvatures required for individual patients. Just because a lens is produced on a digital lathe, it does not insure that it will perform properly. For best results, individualized (or “as worn”) lens designs should be used, and doctors should be careful to test with the patient’s lines-of-sight passing through the optical centers and at right angles (i.e., normal to the test lenses’ surfaces). Measurements should be supplied with every individualized design, and your lab will supply you with a compensated (or as-measured-in-a-lensometer) Rx so you can verify the finished lenses. Using a manufacturer’s pre-selected values for wrap, vertex and pantoscopic tilt, especially when your patient wants frames with significant wrap is not a good idea. If you stop and think about it, would you use a manufacturer’s pre-selected PD and expect top-notch performance?
CAVEAT VIATOR
When helping your patient select frames, caveat viator (seller beware) is a good rule, and this is especially important with wrap frames. There are mechanical and optical limitations that will apply. Unfortunately patients with very strong prescriptions may hear the siren’s song of frames on your frame display that are glazed with plano lenses, and they may insist on a frame design that will ultimately be disappointing in appearance and unsatisfactory in performance. You and your practice bear the responsibility for such situations, and it is usually your reputation that ultimately suffers if a patient’s demands are allowed to override your knowledge and expertise.
If you are not sure that the combination of the patient’s anatomy, prescription and frame of choice will work, it is good practice to caution the patient that the lab’s calculations must be carried out before anyone can be certain that their prescription can be ground and fitted successfully in their frame of choice. Your lab should be able to give you recommended guidelines for base curve and wrap limitations on request if you supply the frame information along with the Rx, PDs and amount of wrap.
Wrap frames offer both cosmetic and practical advantages. They have style, panache and great appeal for many patients. With the ever-growing numbers of people with dry eye problems and increasing awareness of the negative effects of ultraviolet exposure, there will be more and more interest in these frame designs. With just a little extra care when ordering (e.g., asking your lab to be sure to do any needed prescription, prism and PD compensations), wrap frames can offer excellent function and appearance, and patient satisfaction.
Contributing editor Palmer R. Cook, OD, is director of professional education at Diversified Ophthalmics in Cincinnati, Ohio.