


Reprinted from 2020 CE course with permission
What’s Causing The Increase In Myopia?
Here the experts rarely all agree, Most feel that parental genetics are important in determining whether any individual becomes myopic, but in view of the worldwide increase in myopia, researchers often place genetics behind these common suspects:
- An increase in the amount of time children spend on close-focus activities
- An increase in the amount of time spent using mobile devices
- A decrease in the amount of outdoor activities under bright sunlight
- The newly-recognized importance that peripheral retinal blur can initiate processes resulting in increased axial growth.
Let’s look at these factors one by one:
- Increase in close-focus activities: Although not universally agreed upon, many myopia experts feel that the increased accommodative tension encountered during sustained close focus tasks weakens aspects of the scleral attachment to the ciliary body, thereby allowing it to stretch or elongate.
- Increased use of mobile devices: These devices, which are typically held 3 to 4 inches closer to the eye than the normal distance of 16 inches, place additional accommodative and convergent demands on the eye. It is also thought that the light emissive nature of mobile device screens may produce a negative compounding effect on the peripheral retinal images during close tasks and perhaps stimulate axial growth.
- Decreased outdoor activities: Here theories infer that exposure to sunlight narrows the pupil and therefore reduces peripheral blur through the pinhole effect. Other studies suggest that some wavelengths of sunlight have a beneficial effect by increasing retinal dopamine production, which is thought to help meditate axial growth. There appears to be a correlation between the weekly hours children spend in sunlight activities and the degree of myopic progression.
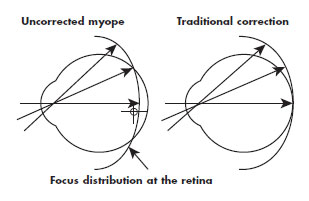
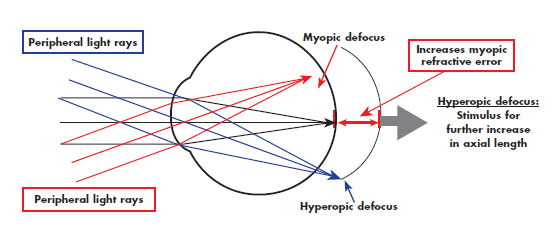
- Peripheral hyperopic induced blur: The peripheral image shell formed in the eye of a well-corrected or under-corrected myope through the use of best form lenses is hyper-opic in nature and therefore found behind the retina. As the peripheral retina’s photosensitive and processing cells have evolved to seek images with the best edge gradients and highest contrast, mechanisms in the eye have been created that automatically try to extend the peripheral retina rearward in order to obtain optimal contrast in the image plane. The end result is an axial elongation of the rear scleral shell, resulting in increase in myopia.
Controlling The Myopic Progression
When measuring the efficacy of myopia-controlling treatments, today’s researchers are using a metric based on quantifying and comparing changes in the axial length of the eye or more specifically, the change in the depth of the vitreous chamber. Amongst the most important current tenants in research surrounding myopia control is that one cannot completely stop the myopic progression. Below is an overview of the primary treatment avenues that researchers have investigated in their efforts to slow or arrest the rate of myopic progression:
- Relieving accommodative effort: Historically, both bifocal and progressive spectacle lenses have been employed to reduce the myopic progression by targeting a reduction in accommodative effort, albeit with mixed results. Parents have often intuited that under correcting the myopic error in spectacles would reduce its progression, but studies have shown that not only is this largely ineffective, it has, in many cases, actually increased the total myopia observed. Alternately, bifocal contact lenses have been shown to offer statically significant reductions in the rate of myopic progression in many studies (see Ortho K below).
- Reducing the neuro-retinal triggers stimulating axial growth: With respect to reducing peripheral hyperopic blur as a key trigger, spectacle lenses have been developed that employ an alternate peripheral aberration correction and have been shown to be a statistically-significant treatment in reducing myopic progression, Carl Zeiss distributes a version of this lens, called MyoVision, in various markets around the world, but not currently the United States. Additionally, progressive and bifocal contact lenses have been specifically used to target reducing peripheral hyperopic blur and have delivered clinically significant results.
Corneal reshaping: Known variously as Orthokerantology (OK), Ortho-K, Corneal Reshaping Treatment (CRT) and Vision Shaping Treatment (VST), this modality uses a rigid, reverse-geometry design, oxygen-permeable contact lens that is worn overnight. It is designed to flatten the central cornea while steepening the periphery, thereby simultaneously attempting to deliver an improved foveal focus while reducing peripheral hyperopic blur. Overall, studies have shown up to a 40 percent reduction in axial length gain through corneal reshaping treatment.
Anti-Muscarinic Therapy: Atropine and pirenzepine are also thought to mitigate the action of the neural-retinal growth trigger in the scleral shell. These drugs, however, even in low dosages sometimes produce unwanted side effects in selected individuals. Their long-term efficacy for use with children is unknown.
The Evidence Is Clear
In view of the documented negative health, behavioral and economic impact portended by the worldwide increase in the incidence of myopia, it is essential that all eyecare professionals and staff, from eye doctors to healthcare technicians to even dispensary personnel, keep up with the latest information on controlling myopic progression in children. The following studies stand out and merit your attention: the Correction of Myopia Evaluation Trail (COMET); Children's Overnight Orthokera-tology Investigation (COOKI); The Contact Lens and Myopia Progression study (CLAMP); the Corneal Reshaping and Yearly Observation of Nearsightedness study (CRAYON); the Longitudinal Orthokeratology Research in Children study (LORIC) and the forthcoming Stabilization of Myopia by Accelerated Reshaping Technique trial (SMART).
Understanding and early intervention is the key toward addressing the world’s growing myopia epidemic.
The journey to realizing the joys and rewards of helping reduce the negative impact of myopia are easy for both parents and professional, and begins at www.myopiaprevention.org.
Special thanks to Dr. Saulius Varnas and Dr. Stephen Silberberg for their help and time taken to provide their expertise on the science of myopia control.

Barry Santini graduated from New York Technical College in 1975 with an AAS in Ophthalmic Dispensing. He is a New York State licensed optician with contact lens certification, is ABO certified and was awarded an ABO Master in 1994. As sales manager for Tele Vue Optics from 1987 to 2003, Santini developed his knowledge of precision optics and has been an owner of Long Island Opticians in Seaford N.Y. from 1996 to present. In addition, Santini is an amatuer astronomer and lecturer and plays bass trombone in the Brooklyn Symphony.







