Either of these conditions can potentially induce significant differences in the prism created as the eyes move up and down when looking through lenses. The difference in the prism is called vertical imbalance. For example, patients viewing objects in their field of view with chin down, through the upper portions of the lenses, view the world through prism. If the lenses are of different powers (as most prescriptions are), then an imbalance in prism is created.
Any imbalance created can be reduced by raising their chin until there is minimal residual imbalance (less than 0.5 prism diopters). In single vision lenses, the patient can simply raise or lower their chin to look along the optical axis, where no deviation takes place. However, when dispensing a pair of multifocals, the patient is required to look through a location in the lens when reading, typically in the lower half, that is a significant distance away from the point of no prism – the distance OC. The patient is now effectively viewing the object through a prism and prismatic deviation occurs. As discussed earlier, this deviation is dependent on the lens power and the distance from the OC to the position in the lens through which the eyes are looking.
The direction of displacement is dependent on whether the lens is “plus” or “minus.” When looking down from center, a “plus” lens induces a BU prismatic effect and the image appears to shift downwards; a “minus” lens induces a BD effect and the image appears to shift upwards. As an industry standard, a distance of 10mm below the distance OC is assumed for the point in the lens used for near work.
Calculating Vertical Displacement at the near point (NP)
Once again, using Prentice Rule:
Prismatic effect at NP = Lens Power vertically (90th meridian) x Distance from OC (cm)
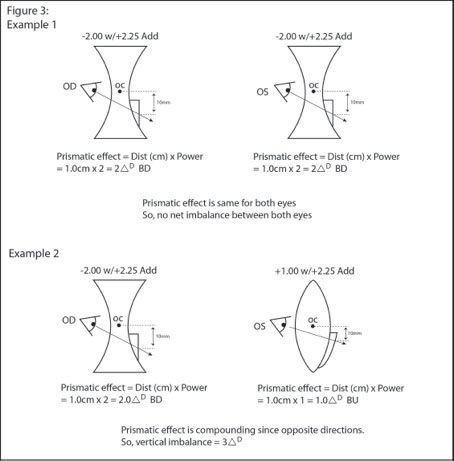
Vertical imbalance affects stereopsis at the NP making near tasks difficult. Depending on the amount of imbalance, the patient can sometimes compensate for it. However, over time this can cause headaches and eye strain.
How much imbalance is too much?
The patients most often affected by vertical imbalance are multifocal wearers with good visual acuity in both eyes and an imbalance greater than 1.5D. When a patient only has good vision in one eye, this eye dominates and the brain suppresses the weaker eye. Therefore, any vertical imbalance present in the written prescription will not actually translate to becoming a vision problem for the patient.
NOTE: Correcting for induced vertical imbalance is especially critical when it is of recent onset. For example, following cataract, or refractive surgery on one eye only.