

The Many Facets of Prism In Ophthalmic Lenses
By Kai Rands, ABO-AC
Learning Objectives:
Upon completion of this course participants will be able to:
- Describe basic prism optics in ophthalmic lenses relative to vergence, deviation and displacement of light
- Explain wanted versus unwanted prism in a lens - prescribed prism versus induced prism from centration errors
- Discuss ocular conditions and therapeutic uses for which prism might be prescribed
- Describe how prism in a lens can be created through centration
- Explain how a lab converts rectangular coordinates to polar coordinates to resolve for resultant prism degree
- Discuss prism verification in ophthalmic lenses
Faculty/Editorial Board
 Kai Rands is a North Carolina licensed and ABO/NCLE-certified optician at Ocutech, which manufactures vision enhancing systems such as bioptic telescopes. Kai received a Durham Tech Opticianry AAS Degree, and holds a B.S. a Masters of the Arts and a Doctorate of Philosophy and Education. Kai has experience as a vision neuroscience researcher as well as extensive expertise in education higher education, public schools, and community programs. Kai also works as an independent scholar and educational service provider.
Kai Rands is a North Carolina licensed and ABO/NCLE-certified optician at Ocutech, which manufactures vision enhancing systems such as bioptic telescopes. Kai received a Durham Tech Opticianry AAS Degree, and holds a B.S. a Masters of the Arts and a Doctorate of Philosophy and Education. Kai has experience as a vision neuroscience researcher as well as extensive expertise in education higher education, public schools, and community programs. Kai also works as an independent scholar and educational service provider.
Credit Statement
This course is approved for one (1) hour of CE credit by the American Board of Opticianry - ABO, Ophthalmic Technical Level 3, Course STWJHI077-3
Support
This course is supported by an educational grant from ZEISS.
 This free CE course is sponsored by ZEISS through an educational grant. ZEISS has strong commitment to the education of opticians dating back as early as 1908, when the Carl Zeiss Foundation approached the German Association of Ophthalmic Opticians (DOV) with the proposal that a specialist school should be set up for ophthalmic opticians. The profession of “ophthalmic optician” came into being in Germany in the late 1920s and is inextricably linked to ZEISS’ quest for improved and standardized training for opticians. ZEISS recognizes that the evolving and highly technical advancement in ophthalmic lens science requires the modern optician to have a solid background in basic optics while keeping abreast of the newest technologies available in the casting and manufacture of lenses for eyeglasses.
This free CE course is sponsored by ZEISS through an educational grant. ZEISS has strong commitment to the education of opticians dating back as early as 1908, when the Carl Zeiss Foundation approached the German Association of Ophthalmic Opticians (DOV) with the proposal that a specialist school should be set up for ophthalmic opticians. The profession of “ophthalmic optician” came into being in Germany in the late 1920s and is inextricably linked to ZEISS’ quest for improved and standardized training for opticians. ZEISS recognizes that the evolving and highly technical advancement in ophthalmic lens science requires the modern optician to have a solid background in basic optics while keeping abreast of the newest technologies available in the casting and manufacture of lenses for eyeglasses.
An optical prism is a transparent three-dimensional object, typically made up of flat faces which form a polyhedron. Optical prisms are used to separate white light into the electromagnetic radiation spectrum (dispersion), change the direction of light rays (deviation), shift a laser beam laterally without changing its direction (displacement) or change the orientation of images (rotation). Some prisms perform more than one of these functions. Dispersion prisms are often one component of spectrophotometers. Spectrophotometers measure how much light at different wavelengths is absorbed by tinted lenses and other materials. Deviation prisms are used in some types of bioptic telescopes to redirect light through the telescope from the object to the eye. Bioptic telescopes are frame mounted telescopes for people with low vision. Displacement prisms are used in binoculars. A type of rotation prism is used in the slit lamp.
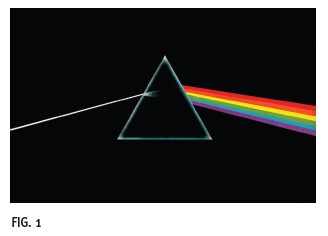
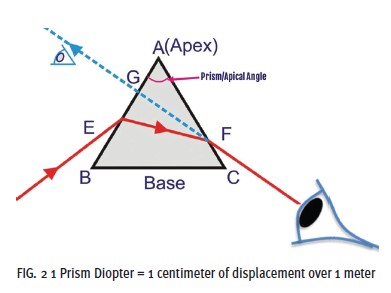 The type of prism most relevant to ophthalmic lenses is similar to the iconic prism seen on Pink Floyd’s Dark Side of the Moon album cover. The cross-section of the triangle in the album’s image illustrates the base of the triangle along the bottom edge and its apex at the top. In this illustration, white light enters the prism as a single beam and emerges as the visible light spectrum, showing one of the prism’s functions, the dispersion of white light into its component colors (Fig. 1). The prism also deviates light toward the prism base and displaces the image viewed in the direction of the prism apex. Suppose a light ray containing only a single color (wavelength) passes through the triangular prism. The single-wavelength light beam will not disperse but will deviate toward the prism base, as seen in Fig. 2. Part 1 of this course focuses on the ways in which prism in ophthalmic lenses can be used to benefit patients with ocular and systemic conditions.
The type of prism most relevant to ophthalmic lenses is similar to the iconic prism seen on Pink Floyd’s Dark Side of the Moon album cover. The cross-section of the triangle in the album’s image illustrates the base of the triangle along the bottom edge and its apex at the top. In this illustration, white light enters the prism as a single beam and emerges as the visible light spectrum, showing one of the prism’s functions, the dispersion of white light into its component colors (Fig. 1). The prism also deviates light toward the prism base and displaces the image viewed in the direction of the prism apex. Suppose a light ray containing only a single color (wavelength) passes through the triangular prism. The single-wavelength light beam will not disperse but will deviate toward the prism base, as seen in Fig. 2. Part 1 of this course focuses on the ways in which prism in ophthalmic lenses can be used to benefit patients with ocular and systemic conditions.
 BINOCULAR VISION
BINOCULAR VISION
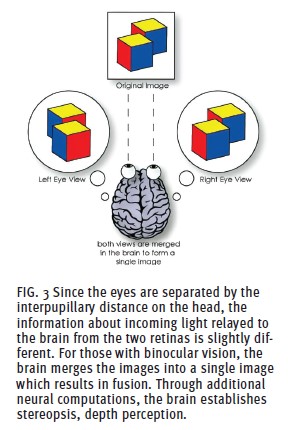
Binocular vision relies on the interaction between light rays, retinal neural networks and visual pathways within the brain. Because our eyes are separated on the face by the interpupillary distance, there is a discrepancy in the information relayed to corresponding photoreceptors between the two eyes. Yet, those with binocular vision see a single image, as seen in Fig. 3. Binocular vision involves three sensory (afferent) perception levels: macular perception, fusion and stereopsis. In macular perception, the visual axis of each eye connects the object to the fovea through the center of rotation of the eye. Fusion occurs further along the visual pathways and results in the perception of a singular image. Stereopsis, the highest grade of binocular sensory perception, involves complex computations within the visual pathways to analyze the location of objects in three-dimensional space. “Stereopsis involves both fusion and suppression processes. The fusion process constructs a stereo percept by integrating the inputs from similar features in the images seen by the two eyes. At the same time, dissimilar inputs are suppressed to promote a single binocular percept.” (Irina Sverdlichenko, et al, onlinelibrary.wiley.com/ doi/full/10.1111/opo.12925)
Binocular sensory perception and eye movements must coordinate so the visual axes converge on the target object at the right time. The physiology involved is more complex than sensory input driving motor (efferent) responses or vice versa. The process involves interaction between afferent and efferent pathways. Extraocular muscles play an important role in converging and diverging the visual axes. The medial rectus muscles contract for convergence while the lateral rectus muscles relax. In divergence, the lateral rectus muscles contract while the medial rectus muscles relax. Nerve fibers innervating these muscles must maintain balanced tension, or tonicity, between the extraocular muscles for the muscles to coordinate. In ideal binocular vision, vergence responses also coordinate with accommodation to keep the image clear.
PRISM FOR BINOCULAR VISION DISORDERS
Binocular vision dysfunction (BVD) can occur at any point in coordinating eye movement, accommodation and sensory processing. Tropias and phorias involve misalignment of the visual axes. Manifest tropias are always present. Intermittent tropias are only apparent some of the time. Tropias are also referred to as strabismus. Phorias last a very short time. Researchers and clinicians have developed scales to rate eye turn duration from pure phoria to manifest tropia, as described in Clinical Management of Binocular Vision by Mitchell Scheiman and Bruce Wick. Tropias and phorias can involve eye turns that are in (esotropia, esophoria), out (exotropia, exophoria), up (hypertropia, hyperphoria) or down (hypotropia, hypophoria). Eyecare professionals can use prism to displace the image to influence the viewer’s perception. There are two overarching approaches to using prisms to treat tropias and phorias. Relieving prism displaces the image toward the viewer’s visual axes. In other words, relieving prism relieves the neural and muscular effort required to maintain fixation on the target. The base is placed on the opposite side as the deviation for relieving prism. For example, the eye tends to turn inward in esophoria, so a base-out prism is used. Adverse prism has the opposite effect. By making it more challenging to maintain fixation, adverse prism requires neural adaptation and muscular strengthening. For an adverse prism, the base is placed in the direction of the deviation. The adverse prism for esophoria consists of a base in prism. Adverse prism is often used in vision therapy.
Small phorias have not traditionally been considered problematic and are common. Most people tend to have a small exophoria. The expected mean adult horizontal deviation at distance is 1 prism diopter with a standard deviation of +/-1 prism diopter. This means that approximately 68 percent of the population has a horizontal deviation of 0 prism diopters (orthophoria) to 2 prism diopters exophoria based on the statistical normal distribution. The expected adult mean horizontal deviation at near is 3 prism diopters exophoria with a standard deviation of +/3 prism diopters. Approximately 68 percent of adults have 0 prism diopters (orthophoria) to 6 prism diopters exophoria at near.
Sometimes, a patient’s phoria is within the typical range for distance but outside the range at near or vice versa. The phorias of the two eyes might still be equivalent to one another for distance vision and equivalent at near. In this case, the patient’s eyes are converging too much (convergence excess) or too little (convergence insufficiency) or diverging too much (divergence excess) or too little (divergence insufficiency). In addition to visual symptoms such as blur and diplopia, vergence excesses and insufficiencies are often associated with asthenopia, burning and tearing, and somatic discomfort such as headaches.
PRISM FOR ANISOMETROPIA INDUCED VERTICAL IMBALANCE IN OPHTHALMIC LENSES
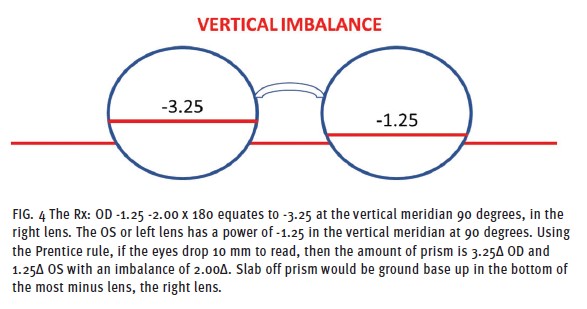
Vertical prism imbalance influences the prismatic effect of image displacement in an ophthalmic lens, where the image appears in space and time for each eye. Significant differences in displacement between right and left lenses can result in diplopia (double vision) and prevent the brain from fusing the two disparate images into one clear image (Fig. 4). A significant difference in the lens power between the right and left lens means the patient has unequal (anisometropia) or opposite (antimetropia) refractive power. When both eyes focus on the object while looking through the lens’ optical center, the brain receives the correct images from both eyes, as both eyes see the same thing in the same place and at the same time. There is no prism at the optical center of the lenses. A vertical prism imbalance is typically experienced when the wearer looks down (away from the lens’ optical axis) to utilize the reading zone in a multifocal lens. Slab-off prism is used to compensate for vertical prism imbalance experienced when the eyeglass wearers’ lenses have a significant difference in power between right and left lenses. The amount of compensating prism is produced on the bottom portion of one of the lenses. A slab off prism is a base-up prism applied to the most minus lens, while reverse slab off prism is a base down prism applied to the most plus lens. Slab off and reverse slab off allow those with significant refractive error differences between the two eyes to fuse images when performing near tasks.
PRISM FOR TRIGEMINAL DYSPHORIA
Researchers are currently investigating whether smaller, more typical phorias are associated with painful conditions such as headaches and neck tension. Some studies have found that pressure on trigger points on extraocular muscles may be related to headache pain. The sensory nerve innervating the lateral rectus muscle is the supraorbital branch of the trigeminal nerve. It is believed that disorders of the lateral rectus muscle can relay sensory information interpreted as tension headaches. The sense of pain may also arise when the supraorbital branch stretches in uncommon ways. Such pain from nerve stretching, termed mechanosensitivity, could occur due to small phorias or misalignments of the eyes. The nerve could also over-stretch when binocular coordination is disrupted. Use of screens such as computers, phones and tablets may exacerbate symptoms when the supraorbital branch maintains a particular position over an extended period of time. Since other symptoms such as asthenopia, neck and shoulder pain, dizziness, dry eye sensation and light sensitivity seem to cooccur with headaches, it is possible that this cluster of symptoms may have similar underlying mechanisms. This group of symptoms has recently been referred to as trigeminal dysphoria.
Since most people have less misalignment at distance than at near, the amount of prism in a contoured lens typically increases gradually from distance to near. The change is tailored specifically to the needs of each patient. Contour prism lenses have been compared to progressive lenses: Progressive lenses gradually vary the add power, while contour prism lenses gradually vary the amount of prism.
PRISM FOR AUTOIMMUNE DISEASES
Autoimmune diseases can affect eye motility and binocular vision. Graves Eye Disease, also known as Thyroid Eye Disease, is an autoimmune disease in which thyroid stimulating hormone receptor antibodies bind to receptors on the surface of cells including cells in the extraocular muscles. Typically, the first target of the antibodies is the inferior rectus and inferior oblique muscles followed by the lateral rectus. As the antibodies bind with receptors, the extraocular muscle cells become inflamed. Inflammation leads to tropias often causing diplopia. The inflammation can also inhibit extraocular muscle motion, which can cause diplopia as version—the ability of the eyes to turn in the same direction—is differentially affected in the two eyes. As the extraocular muscles expand, the globe is often pushed forward, a sign called proptosis. Proptosis stretches the optic nerve which can eventually lead to optic nerve damage. Vertical or horizontal prism (or a combination of both) can address diplopia caused by the tropias and motility issues involved in Graves Eye Disease.
Myasthenia gravis is an autoimmune condition that affects the junction between nerves and muscles (neuromuscular junctions). Nerves release the neurotransmitter acetylcholine at neuromuscular junctions to stimulate muscle contraction. In myasthenia gravis, acetylcholine receptor antibodies block acetylcholine from binding to receptors in muscles. This dampens muscle reactions and causes muscle weakness. Receptors in the muscle that are not regularly stimulated are removed which leads to progression of the condition. Although myasthenia gravis is a progressive condition, symptoms fluctuate throughout the day and are often worse later in the day. The extraocular muscles (especially the medial rectus), the levator palpebrae superioris (which opens the eyelids) and the orbicularis oculi (which closes the eyelids) are often the first muscles in the body to be affected. Muscle weakness in ocular muscles leads to eye misalignment, motility issues and intermittent diplopia. The effectiveness of prism treatments depends on how much the muscle weakness fluctuates throughout the day.
PRISM FOR MILD TRAUMATIC BRAIN INJURY
Since binocular vision involves not only the eye but also the brain, neurological conditions can affect binocular vision. Mild Traumatic Brain Injury (mTBI), also known as concussion, involves external forces acting on the head resulting in damage to the brain. Falls, vehicular crashes and assault are some of the ways mTBI occurs. Sports-related injuries among athletes and injuries from explosions among military service members can also result in mTBI. Mild Traumatic Brain Injury can affect cranial nerves, extraocular muscles, vergence and eye alignment. Commonly, patients experience diplopia, convergence insufficiency and eye motility issues. Patients often have difficulties with reading following mTBI.
Several syndromes may result following mTBI. Postconcussion Syndrome is when symptoms of mTBI continue for longer than expected. As visual symptoms, blur and diplopia may persist in Postconcussion Syndrome. Prism can be used to address the diplopia as long as this symptom persists.
Researchers and clinicians have proposed that patients may experience Posttrauma Vision Syndrome. Visual and ocular motor dysfunction, it is thought, drives a wide range of other symptoms in cognitive, psychological, musculoskeletal and vestibular systems. The extent to which prism can address these wide-reaching symptoms needs to be confirmed by additional research.
Midline Shift Syndrome involves miscommunication of visual and proprioceptive perception. Proprioception is the sense of how parts of the body are situated and move in three-dimensional space. When visual and proprioceptive information does not match, patients perceive a shift in their subjective midline which can affect gait and balance. Yoked prism has been used to improve patients’ balance. Yoked prism involves a pair of prisms that deviate light in the same direction—both left, both right, both up or both down.
Vertical Heterophoria Syndrome involves a small hyperphoria or hypophoria. Theoretically, these phorias stem from damage to the brainstem or the utricle (an organ that detects when one’s head tilts). The theory related to Vertical Heterophoria Syndrome also needs more supportive evidence. When a patient has a vertical heterophoria after mTBI, base up or base down prism may help alleviate symptoms.
PRISM FOR HEMIANOPSIA
Homonymous hemianopsia is a condition in which patients lose visual function in one vertical hemifield. In other words, patients only see objects positioned on one side of their midline. At the optic chiasm, some axons from the left and right optic nerves cross the midline regrouping the fibers into the left and right optic tracts. The effect is that each optic tract mainly includes fibers from the contralateral eye, separating the two optic tracts by visual field rather than by eye. Hemianopsia often occurs from damage to one of the optic tracts. The condition can also result from damage to the optic radiations or visual cortex. Patients with hemianopsia often collide with other people and objects on the side with the hemifield defect which interferes with mobility.
Peripheral prisms are used to relocate and expand patients’ visual field. Eli Peli, OD, developed an approach he termed vision multiplexing. It is based on the idea from engineering of transmitting multiple messages over the same communication channel at the same time. In multiplexing, the multiple messages can be separated when received. In vision multiplexing, prisms are used to deviate light so that images from the missing hemifield appear within the unaffected hemifield. Fresnel prisms are a series of tiny parallel prisms with all of the bases in the same direction. Using a series of tiny parallel prisms can provide the effect of a single stronger prism with a much lower thickness. For hemianopsia, base out Fresnel prisms are placed in the upper and lower portions of the lens corresponding to the side with the hemifield defect. Patients view through the center portion of the lens to see images from the unaffected hemifield. In their upper and lower peripheral vision, they see images from the missing hemifield. Processing these multiple images at the same time requires training. With practice, many patients’ mobility improves. A peripheral prism design using oblique prisms has also been developed for driving.
PRISM FOR SPATIAL NEGLECT
Spatial neglect is a condition in which patients have difficulty attending to people and objects on one side of their midline.
For example, a patient may only put one side of a jacket on or only eat food from one side of the plate. While in hemianopsia, the patient knows that both sides exist but cannot perceive one hemifield, in spatial neglect, the patient is unaware that one side exists. Hemianopsia and spatial neglect can coexist. Spatial neglect can result from stroke in several areas of the cortex or in axons connecting the cortex to other areas of the brain.
Prism adaptation has been used as a rehabilitation strategy for spatial neglect. In prism adaptation, patients wear lenses with high horizontal yoked prism. For example, patients with left neglect will wear base left prisms that shift the image to the right. Patients then participate in tasks such as grasping an object. At first, patients will reach for the object too far to the right. By comparing their hand movement to the location of the object, patients learn to adjust their hand movements to the left and accurately grasp the object. Once the patients remove the prisms, they continue to reach toward the left—now they are reaching into the previously neglected space on the left side. The same procedure is repeated in subsequent sessions. Over time, neural connections reorganize so that patients are able to better perform daily activities in the neglected space.
PRISM FOR HIGH MAGNIFICATION READING LENSES
Magnification is helpful for many patients with low vision. Low vision is a broad term for visual conditions that interfere with daily activities. If spectacles or contact lenses correcting refractive errors are the only tool needed to address an individual’s visual needs, the person is not considered to have low vision. An example of a condition that may cause low vision is age-related macular degeneration. This condition may cause central scotomas that interfere with distance activities (such as recognizing loved-ones’ faces and driving ) and near activities (such as reading and certain hobbies). Magnification makes an object appear larger so that the scotoma covers up less of the image.
People with other conditions leading to low vision, especially when individuals have corrected visual acuities between 20/60 and 20/300, also benefit from magnification. For example, the macula often does not completely develop for those with albinism. People with diabetic retinopathy may experience macular edema which interferes with central vision. Patients with high myopia are at risk for macular holes in which the vitreous pulls a part of the retina away from the retinal surface. Those with high myopia are also at risk for developing myopic degeneration. In myopic degeneration, retinal cells can atrophy causing visual impairments. Stargardt’s Disease is a form of macular degeneration that typically begins in an individual’s teens or twenties.
Magnification alone often improves visual acuities for distance vision. Magnification also improves visual acuities for many people for near vision tasks. Since plus lenses magnify, high plus reading glasses can enhance vision for near work. Reading caps—plus lenses that slide onto or are affixed to a bioptic telescope—can have a similar effect. Bioptic telescopes are small telescopes mounted on spectacles to serve as a visual aid. During near tasks, the eyes must converge to fixate on a near object. When people’s eyes converge, they look through the nasal portion of the high plus lens which has a high amount of base out prism. The base out prism deviates light out making the image appear closer in toward the viewer. This requires the viewer’s eyes to converge even more leading to discomfort and sometimes diplopia. Incorporating base in prism into the high plus lenses counteracts the need for the eyes to converge excessively and makes near tasks easier. This allows wearers to participate in near tasks for longer periods of time.
PRISM AS A TOOL FOR ENHANCING VISION AND DAILY LIFE
Part 1 has focused on the purpose of prism in eyecare. Eyecare professionals leverage prism to enhance the daily experiences of individuals with a wide variety of conditions. Prism can improve the binocular vision of those with tropias and phorias. Slab off uses prism to allow those with differing refractive errors in the two eyes to fuse images during near tasks. Contoured prism lens design address eye misalignments previously considered within the typical range to improve symptoms for 90 percent of patients treated for binocular vision disorder leading to trigeminal dysphoria. When our eyes are misaligned, we can experience headaches, eyestrain and fatigue, dry eye sensation, neck and shoulder pain, motion sickness/feeling off-balance, poor depth perception, blurred or double vision, difficulty reading, sensitivity to light and even restless sleep. Systemic disorders such as Graves’ disease and myasthenia gravis affect binocular vision. Those with these systemic disorders often benefit from prescribed prism. Innovative uses of prism to provide multiple channels of visual information within the same hemifield reduce collisions for those with hemianopsia. Prism adaptation training prompts neural changes that improve attention to neglected space in those with spatial neglect. Prism in conjunction with high plus reading lenses allows many people with low vision to participate in near activities such as reading and hobbies. Part 2 will investigate the optics of prism in ophthalmic lenses, and the role of optical labs and dispensing opticians in producing and verifying lenses with and without prescribed prism.

